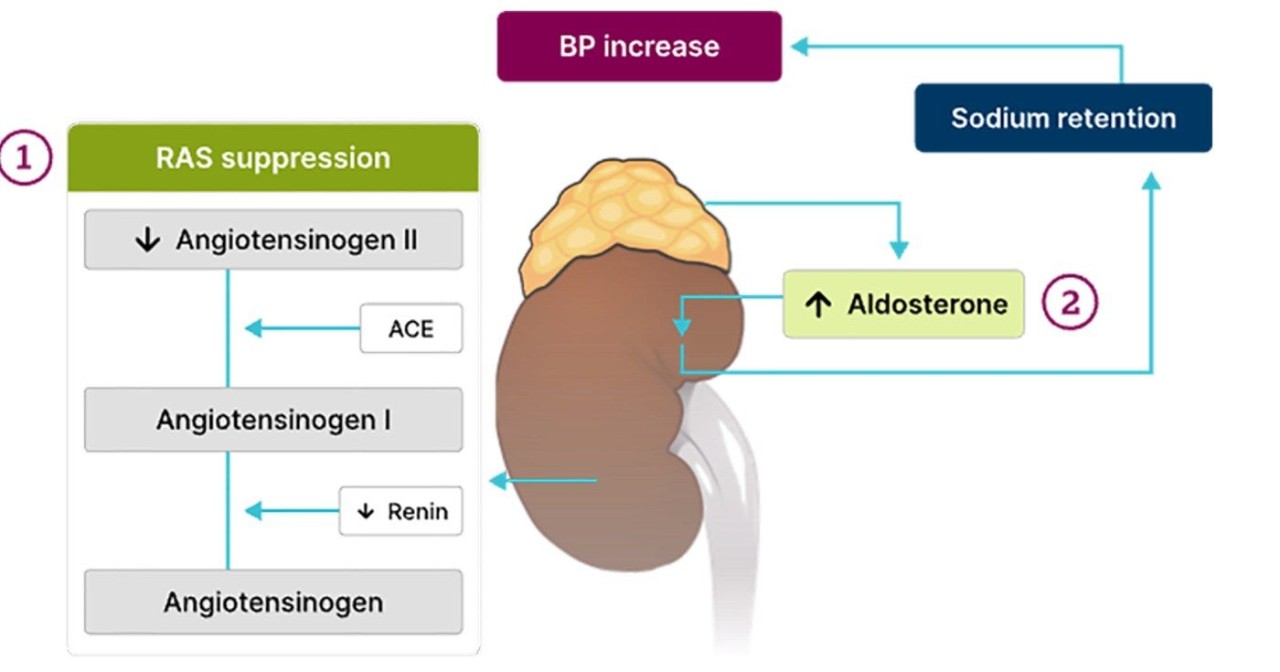
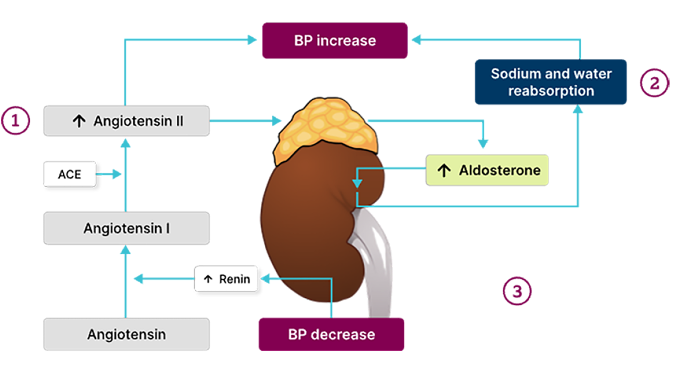



Feedback loop2,3
Elevations in BP and sodium lead to:
- Inhibition of renin release
- Decreased RAAS activation
- Reduced aldosterone production

References
1. Bioletto F, Bollati M, Lopez C, et al. Int J Mol Sci. 2022;23(9):4803.
2. Brown JM, Siddiqui M, Calhoun DA, et al. Ann Intern Med. 2020;173(1):10-20.
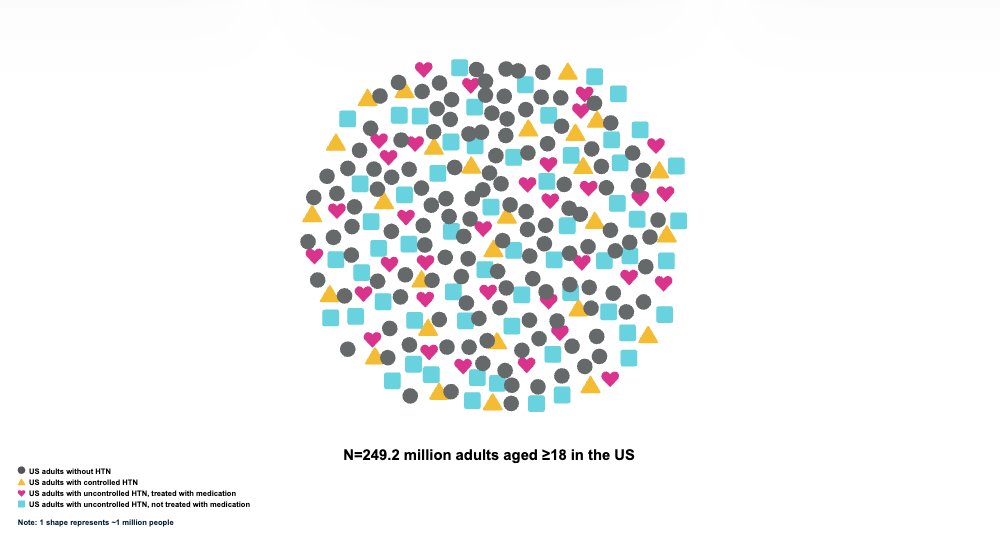
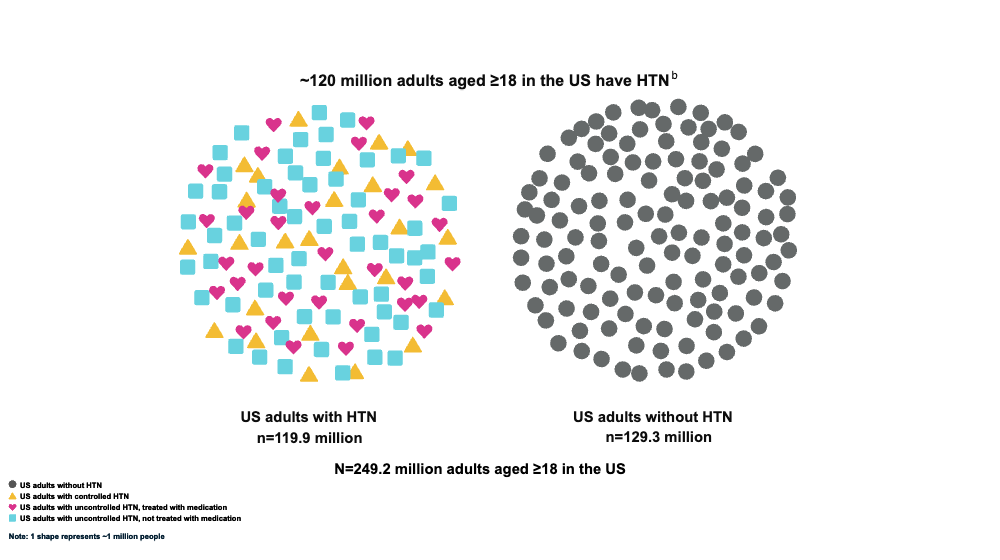
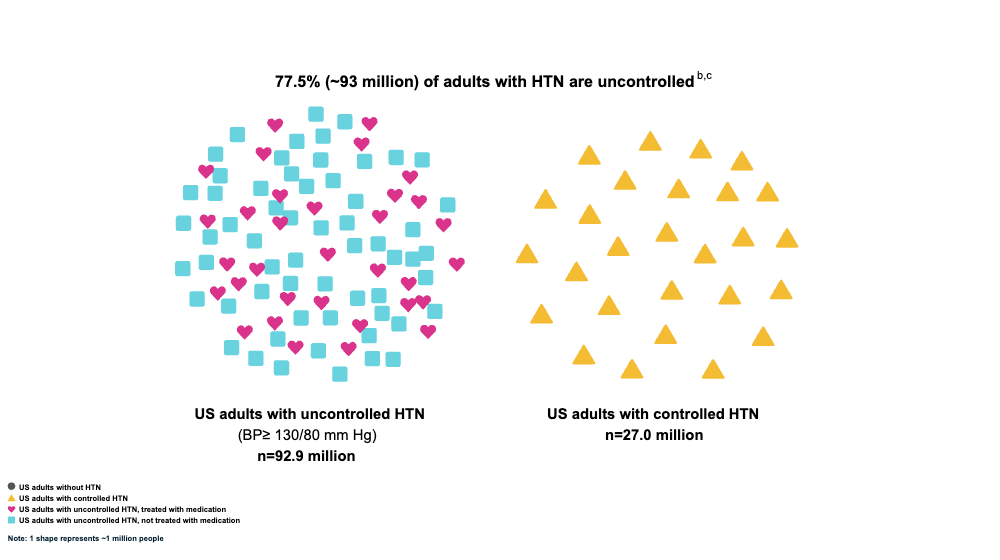
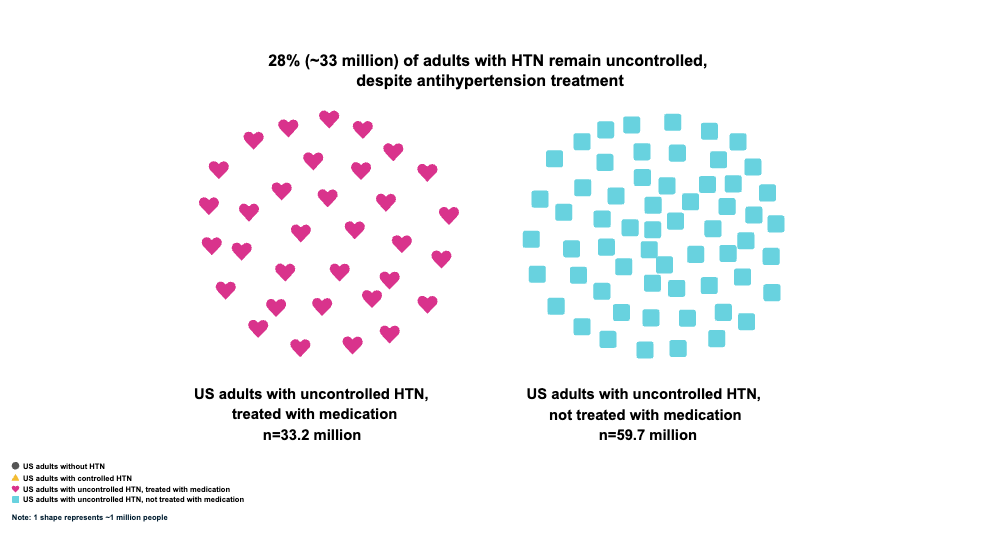
Note: 1 shape represents ∼1 million people.
aHTN prevalence and control estimates among US adults aged ≥18 years, applying criteria from the ACC/AHA 2017 HTN Clinical Practice Guideline utilizing data sourced by NHANES 2017-2020.1
bHTN is defined as a BP ≥130/80 mm Hg or currently using antihypertensive medication.1
cAll adults recommended lifestyle modifications only are considered uncontrolled as their BP is above the threshold.1
aProspective cohort study of US adults aged ≥18 years (N=13,947) enrolled in the third National Health and Nutrition Examination Survey (NHANES III) (1988–1994; median follow-up of 19.1 years). HR (95% CI) for the outcomes of all-cause mortality=1.62 (1.35-1.95), cerebrovascular-specific mortality=3.01 (1.91-4.73), heart disease-specific mortality=2.19 (1.57-3.05), and CVD-specific mortality=2.23 (1.66-2.99).3
| ACC | American College of Cardiology |
| AHA | American Heart Association |
| BP | blood pressure |
| CI | confidence interval |
| CVD | cardiovascular disease |
| HR | hazard ratio |
| HTN | hypertension |
| NHANES | National Health and Nutrition Examination Survey |
| US | United States |
1. Million Hearts. Estimated hypertension prevalence, treatment, and control among U.S. adults. Million Hearts website. https://millionhearts.hhs.gov/data-reports/hypertension-prevalence.html
2. Centers for Disease Control and Prevention (CDC). High blood pressure facts. CDC website. https://www.cdc.gov/high-blood-pressure/data-research/facts-stats/index.html
3. Zhou D, Xi B, Zhao M, et al. Uncontrolled hypertension increases risk of all-cause and cardiovascular disease mortality in US adults: the NHANES III Linked Mortality Study. Sci Rep. 2018;8(1):9418. https://doi.org/10.1038/s41598-018-27377-2
aBased on diagnosis of primary aldosteronism caused by renin-independent aldosterone production. Suppressed renin is defined as low levels (seated: <1.0 mcg/L/hr, supine: <0.6 mcg/L/hr) in the setting of high sodium balance.5
bHigh sodium balance is defined as 200 milliequivalents of sodium daily.6
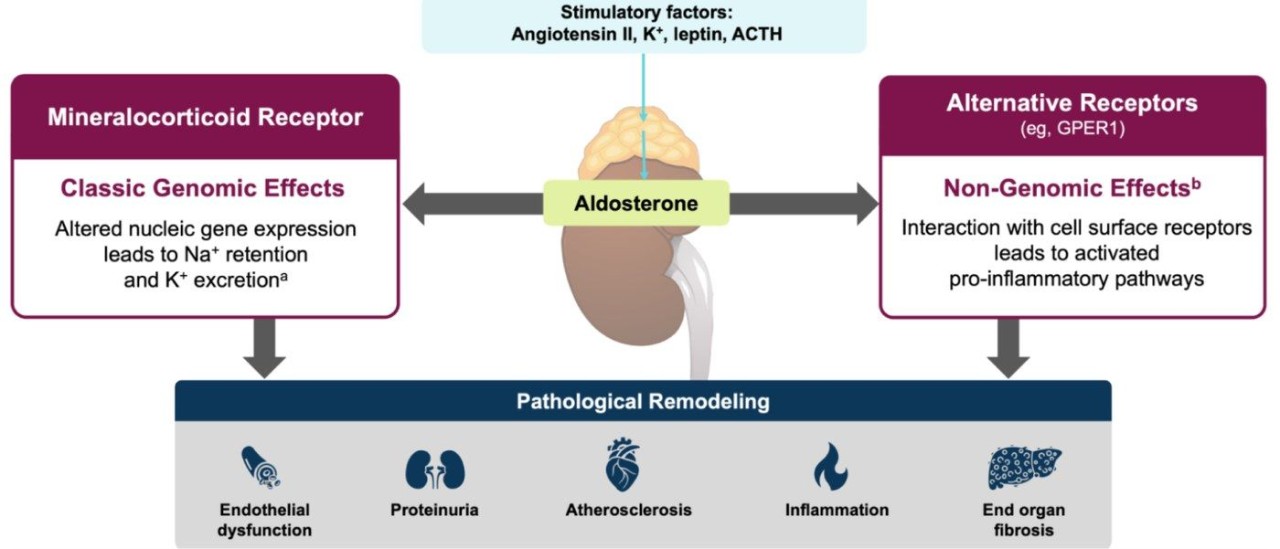
aOccurs within the distal tubules and collecting ducts of the kidney. MRs are expressed in epithelial cells (eg, kidneys, bowel, salivary glands) and non-epithelial tissues (eg, vascular and skeletal smooth muscle, immune system cells, vascular endothelium, cardiac myocytes, and adipocytes).1
bNon-genomic effects can also regulate Nat+/K+ channel activities.7
Association Between Serum Aldosterone Concentrations and BP at Baseline.9,a,b
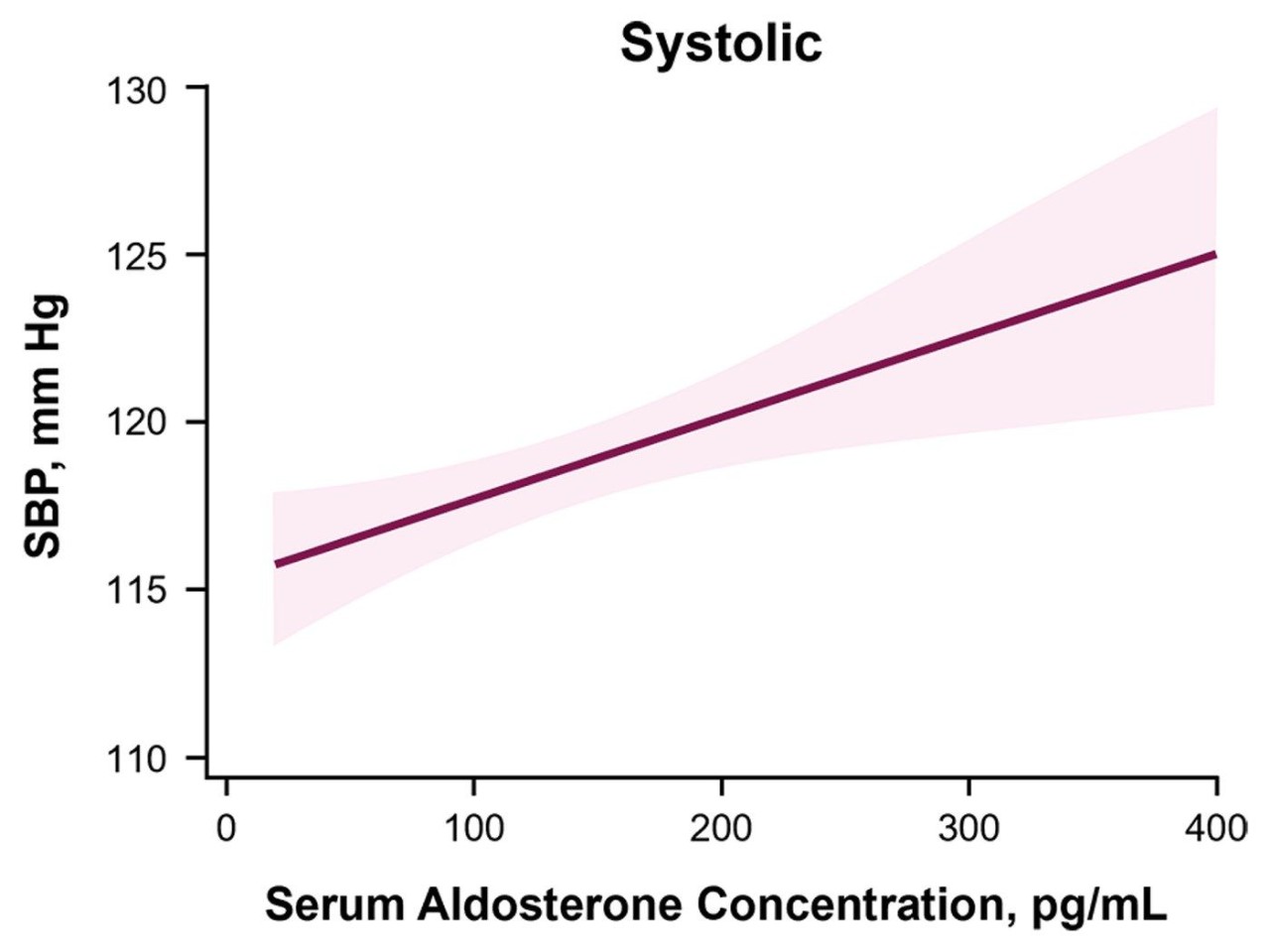
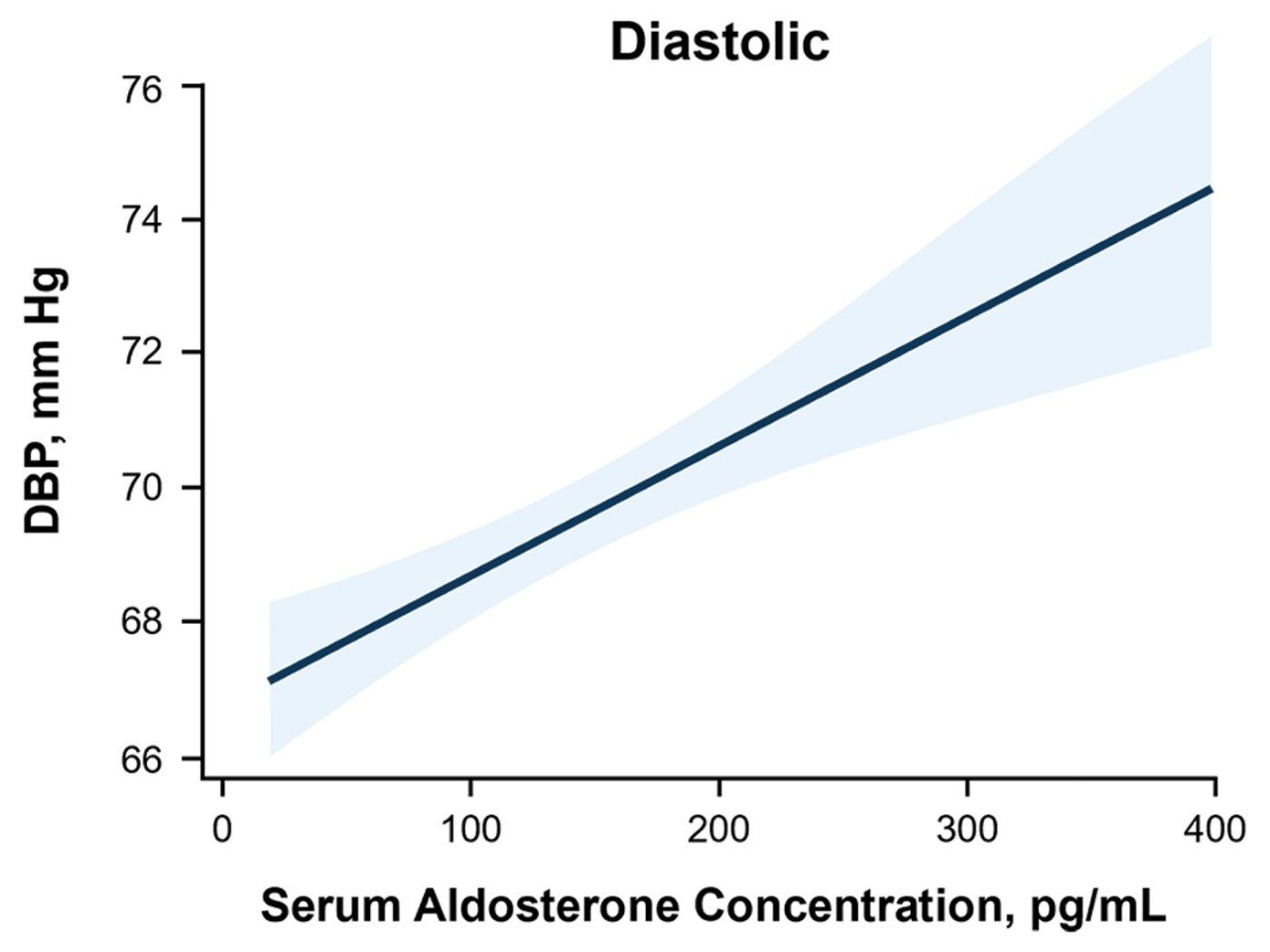
aStudy included 948 US adults (46 to 88 years of age) from the multicenter longitudinal cohort Multi-Ethnic Study of Atherosclerosis (MESA), recruited between July 2000 and August 2002, with follow-up through July 2015. Participants had measurements of serum aldosterone collected and had not taken antihypertensive medications. Results displayed represent the cohort of 700 participants who had follow-up coronary computed tomography scans.9
bAdjusted for age, sex, CAC at Exam 2 or 3, race, education, insurance status, income, smoking status, alcohol intake, physical activity, statin prescription, BMI, LDL, serum and urinary potassium, serum and urinary sodium, and plasma renin activity.9
| ACE | angiotensin-converting enzyme |
| ACTH | adrenocorticotropic hormone |
| BMI | body mass index |
| BP | blood pressure |
| CAC | coronary artery calcium |
| CV | cardiovascular |
| DBP | diastolic blood pressure |
| GPER | G protein-coupled estrogen receptor |
| HTN | hypertension |
| K+ | potassium |
| LDL | low-density lipoprotein |
| MR | mineralocorticoid receptor |
| Na+ | sodium |
| RAAS | renin-angiotensin-aldosterone system |
| RAS | renin-angiotensin system |
| SBP | systolic blood pressure |
| US | United States |
1. Crompton M, Skinner LJ, Satchell SC, et al. Aldosterone: essential for life but damaging to the vascular endothelium. Biomolecules. 2023;13(6):1004. https://doi.org/10.3390/biom13061004
2. Scott JH, Menouar MA, Dunn RJ. Physiology, aldosterone. In: StatPearls [Internet]. StatPearls Publishing; May 1, 2023. https://www.ncbi.nlm.nih.gov/books/NBK470339/
3. Papadopoulou-Marketou N, Vaidya A, Dluhy R, et al. Hyperaldosteronism. In: Feingold KR, Anawalt B, Blackman MR, et al, eds. Endotext [Internet]. MDText.com, Inc.; Last update August 6, 2020. https://www.ncbi.nlm.nih.gov/books/NBK279065/
4. Triebel H, Castrop H. The renin angiotensin aldosterone system. Pflügers Arch - Eur J Physiol. 2024;476:705-713. https://doi.org/10.1007/s00424-024-02908-1
5. Brown JM, Siddiqui M, Calhoun DA, et al. The unrecognized prevalence of primary aldosteronism: a cross-sectional study. Ann Intern Med. 2020;173(1):10-20. https://doi.org/10.7326/M20-0065
6. Yuan YE, Haas AV, Rosner B, et al. Elevated blood pressure and aldosterone dysregulation in young black women versus white women on controlled sodium diets. J Clin Endocrinol Metab. 2024;109(2):e773-e779. https://doi.org/10.1210/clinem/dgad512
7. Kritis AA, Gouta CP, Liaretidou EI, et al. Latest aspects of aldosterone actions on the heart muscle. J Physiol Pharmacol. 2016;67(1):21-30.
8. Verhovez A, Williams TA, Monticone S, et al. Genomic and non-genomic effects of aldosterone. Curr Signal Transduct Ther. 2012;7(2):132-141. https://doi.org/10.2174/157436212800376708
9. Inoue K, Goldwater D, Allison M, et al. Serum aldosterone concentration, blood pressure, and coronary artery calcium: the Multi-Ethnic Study of Atherosclerosis [article and online supplement]. Hypertension. 2020;76(1):113-120. https://doi.org/10.1161/HYPERTENSIONAHA.120.15006
10. Bakris G, Chen C, Campbell AK, et al. Association of uncontrolled blood pressure in apparent treatment-resistant hypertension with increased risk of major adverse cardiovascular events plus. J Clin Hypertens (Greenwich). 2023;25(8):737-747. https://doi.org/10.1111/jch.14701
11. Azizi M. Decreasing the effects of aldosterone in resistant hypertension - a success story. N Engl J Med. 2023;388(5):461-463. https://doi.org/10.1056/NEJMe2216143
12. Blazek O, Bakris GL. Novel therapies on the horizon of hypertension management. Am J Hypertens. 2023;36(2):73-81. https://doi.org/10.1093/ajh/hpac111
aMeta-analysis of 31 studies that evaluated cardiovascular risk in patients with primary aldosteronism (n=3838) compared to patients with essential HTN (n=9284). Median duration of HTN was 8.8 years (IQR 6.2-10.7).2
bOR (95% CI) for the outcomes of coronary artery disease=1.77 (1.10-2.83), atrial fibrillation=3.52 (2.06-5.99); heart failure=2.05 (1.11-3.78), and stroke=2.58 (1.93-3.45).2
aMeta-analysis of 46 studies that evaluated risk in patients with primary aldosteronism (n=6056) compared to patients with essential HTN (n=9733).3
bOR (95% CI) for the outcome of proteinuria=2.68 (1.89-3.79).3
cResults depicted are from a multicenter, prospective, observational cohort study (CRIC) of 3680 patients with known CKD, defined as eGFR 20-70 mL/min/1.73 m2, over a median follow-up of 9.6 years. Results were analyzed using a multivariable model adjusted for age, sex, race, clinical center, BMI, diabetes mellitus, SBP, history of CV disease, HbA1c, history of hypercholesterolemia, serum albumin, serum potassium, ACEi/ARB use, loop diuretic use, statin use, smoking, BNP, 24‑hour urine sodium, 24-hour urine potassium, 24-hour urine protein, and baseline eGFR.4
dCKD progression was defined as the composite of 50% decline in eGFR or incident ESKD.4
eRisk of CKD progression=HR, 1.45; 95% CI, 1.22-1.73 for those in the highest quartile of serum aldosterone relative to lowest quartile.4
fRisk of developing ESKD=HR, 1.46; 95% CI, 1.19-1.78 for those in the highest quartile of serum aldosterone relative to lowest quartile.4
| ACEi | angiotensin-converting enzyme inhibitor |
| ARB | angiotensin receptor blocker |
| BMI | body mass index |
| BNP | B-type (brain) natriuretic peptide |
| BP | blood pressure |
| CI | confidence interval |
| CKD | chronic kidney disease |
| CRIC | Chronic Renal Insufficiency Cohort |
| CV | cardiovascular |
| EC | extracellular |
| eGFR | estimated glomerular filtration rate |
| ESKD | end-stage kidney disease |
| HbA1c | glycated hemoglobin |
| HR | hazard ratio |
| HTN | hypertension |
| IQR | interquartile range |
| NO | nitric oxide |
| OR | odds ratio |
| ROS | reactive oxygen species |
| SBP | systolic blood pressure |
| VSMC | vascular smooth muscle cell(s) |
1. Vasan RS, Evans JC, Larson MG, et al. Serum aldosterone and the incidence of hypertension in nonhypertensive persons. N Engl J Med. 2004;351(1):33-41. https://doi.org/10.1056/NEJMoa033263
2. Monticone S, D'Ascenzo F, Moretti C, et al. Cardiovascular events and target organ damage in primary aldosteronism compared with essential hypertension: a systematic review and meta-analysis. Lancet Diabetes Endocrinol. 2018;6(1):41-50. https://doi.org/10.1016/S2213-8587(17)30319-4
3. Monticone S, Sconfienza E, D'Ascenzo F, et al. Renal damage in primary aldosteronism: a systematic review and meta-analysis. J Hypertens. 2020;38(1):3-12. https://doi.org/10.1097/HJH.0000000000002216
4. Verma A, Vaidya A, Subudhi S, et al. Aldosterone in chronic kidney disease and renal outcomes. Eur Heart J. 2022;43(38):3781-3791. https://doi.org/10.1093/eurheartj/ehac352
5. Verhovez A, Williams TA, Monticone S, et al. Genomic and non-genomic effects of aldosterone. Curr Signal Transduct Ther. 2012;7(2):132-141. https://doi.org/10.2174/157436212800376708
This section offers scientific resources related to aldosterone, an underlying key driver of uncontrolled hypertension, including videos and slide decks. Our AstraZeneca Medical team has created this content as an information service for healthcare professionals. Updates are made to the content as new data become available.
| CV | cardiovascular |
| HTN | hypertension |
Are you interested in learning more about aldosterone as a key driver of uncontrolled hypertension? Would you like to meet with someone from the AstraZeneca Medical team to learn more about AstraZeneca’s ambition in transforming care in hypertension? Use the links below to sign up for more information and/or connect with a Medical Science Liaison in your region. You can also connect with us at one of the upcoming congresses listed below.
US-112429 Last updated 5/26
Thank you for signing up!

This site is intended for healthcare professionals practicing in the US.
©2026 AstraZeneca. All rights reserved.
US-107328
Last Updated 4/26
The information provided on this site is intended for use by healthcare professionals practicing in the US. The dissemination of this information may be subject to different medical and regulatory requirements in other countries.
This web site is intended to help healthcare professionals practicing in the US and AstraZeneca authorized persons find scientifically balanced, evidence-based information about AstraZeneca drugs, submit a question, ask for field medical follow-up, and explore links to professional and patient support resources.
Are you a healthcare professional practicing in the United States?